The Loneliness Apparatus

Since the 1970s, clinical researchers have mounted a large body of evidence demonstrating that social ties or the lack thereof play an important role in mortality rates and in disease prevention. The fruit of this research is now coming to bear: the notion of “loneliness” is playing an increasingly prominent role in public health discussions around the world. With urban populations growing and social media commanding attention, social isolation is indeed growing. Policymakers and researchers are rightly asking how loneliness can be measured, and how it should be addressed. But I have a different question: what are the social effects of promoting “loneliness” as a nation-wide messaging device?
This question serves as a fitting introduction to the idea of cultural determinants of health that I will be exploring frequently at Care Culture. In order to look at the cultural ramifications of loneliness rhetoric, we need to understand the full ecosystem of what loneliness means. Instead of taking the so-called “loneliness epidemic” at face value, I propose we examine the loneliness apparatus: the many social institutions, regulatory decisions, policy programs, scientific research, and public messages that are implicated in the concept.
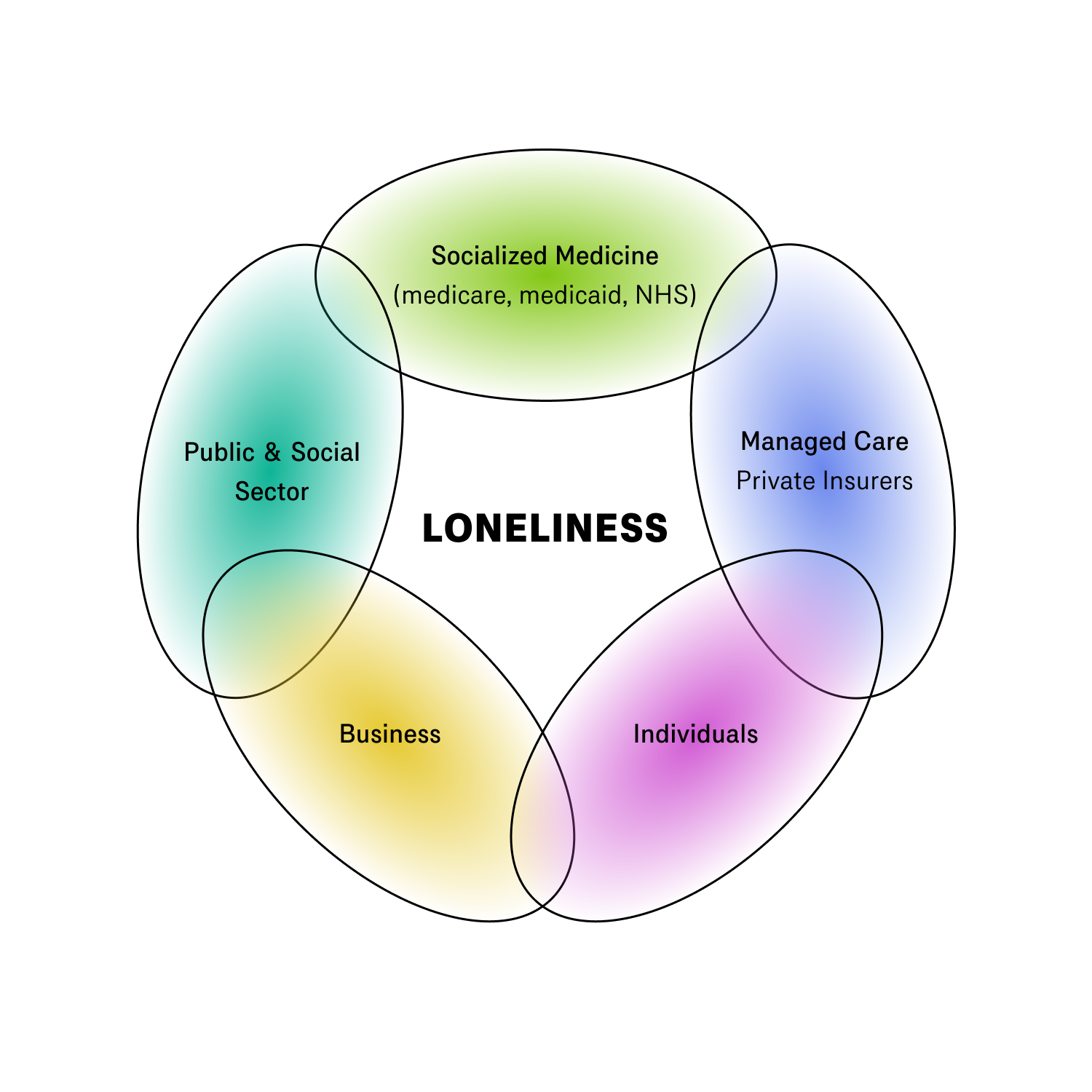
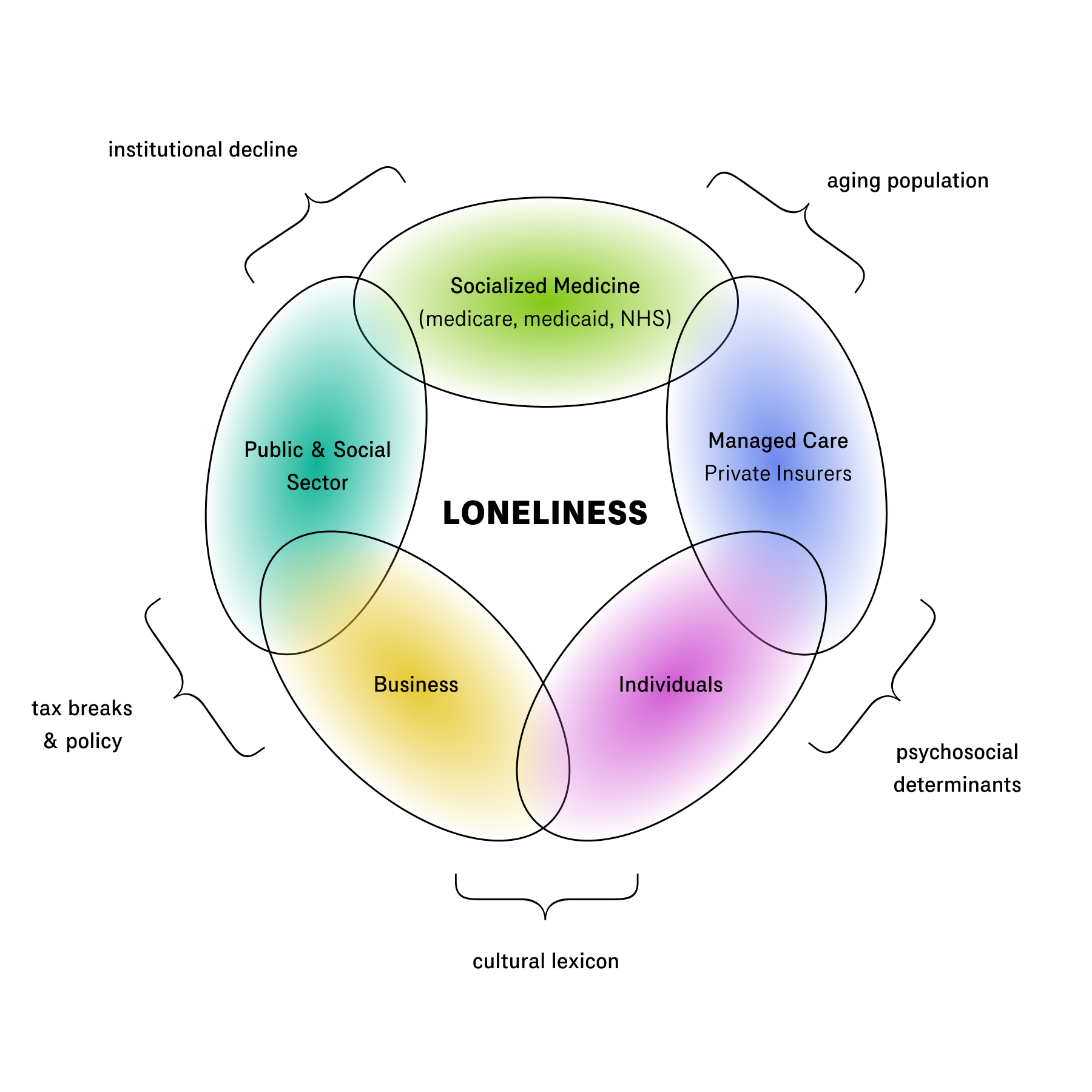
It is easiest to understand what I mean by looking at the different actors involved and their relationship to the apparatus:
- Insurers: government-provided health care and private insurance providers most directly feel the cost burden of loneliness. For these actors loneliness takes two forms: the elderly population, and isolation as a determinant of health among the rest of the population.
- Public Sector: government programs, foundations, and charities are involved with setting loneliness alleviation policies, as well as funding and executing programs. Yet loneliness in this context speaks to issues of public trust and institutional decline.
- Private Sector: as I have documented elsewhere, numerous private organizations now make it their aim to create a sense of belonging, worship, and community. The loneliness apparatus introduces a new dimension to these efforts.
- Individuals: individuals are ultimately those who experience social isolation in their lived realities. The promotion of loneliness as a public health concept may change how they conceive of their own mental health.
While loneliness and mental health are certainly related on the object level, the mental health apparatus and the loneliness apparatus are equipped with different ideas, agendas, and reforms. Once we understand the different parts of the apparatus, we can ask: what job is it trying to do? Are proposed programs likely to succeed? And succeed or not, what do we think will happen when the loneliness propaganda is fully internalized?
1. Insurers
When it comes to promoting loneliness as a public health concept, countries with socialized health care systems lead the charge. Australia, Canada, Denmark, Norway, Sweden, Japan, the UK, among others, have all introduced government-funded programming to address social isolation. The UK has carved out special loneliness responsibilities for an existing government appointment, and Japan created a similar ministership at the height of the Covid pandemic. The colloquial name for these roles across the world is the ominous-sounding “Minister of Loneliness.”
Note that the countries mentioned here are the same ones that come up in discussions of aging demographics. The two issues are closely related, and in some governmental spheres “loneliness” seems to be a circumlocution for “aging population.” Growing urbanization, declining birth rates, and the challenges of multigenerational household zoning mean that the elderly are often relegated to retirement properties with limited access to their families and community. The most studied health risks associated with isolation are chronic diseases like heart disease, cancer, and dementia which disproportionately affect the elderly.
The burden of an aging population weighs heavily on socialized health care schemes. Single payers centralize costs and data. They are generally first in line to take advantage of research on psychosocial health risks in order to reduce overall costs. (This is why California, which operates the largest medicare program in the US, is leading the way in addressing social isolation in the States.) Such expenses include the cost of medicine, emergency treatments and hospital visits, and preventative care, but also the costs of an emerging class of semi-professional care workers. In many countries programs to incentivize elder care work have sprung up, such as CDPAP in New York state. Through these programs, care workers are using medicare budgets.
Private insurers also recognize the health impacts of social isolation and are eager to make loneliness a public theme. Older people are more expensive for private insurers as well, with loneliness being identified as a multiplicative risk factor for chronic conditions. Cigna Group is just one insurance business that has published prolifically on the topic, earning a citation in the Surgeon General’s 2023 report on loneliness. While the online survey methodology used to produce Cigna’s reports is somewhat suspect, it is the fact that Cigna finds this important to publish at all that is notable.
Research on the social determinants of health goes back at least 50 years, yet it is the aging population and the costs it incurs on insurance systems—whether public or private—that now push social isolation and loneliness into the public conversation worldwide.
2. Public Sector
Pressures felt by public health care systems are reflected in policy agendas, public health messaging, and government budgets allocated to address isolation. The Jo Cox Commission’s 2017 report on loneliness in the UK and the Surgeon General’s 2023 Advisory on loneliness in the USA are two artifacts that exemplify the loneliness apparatus. Each cover the problem and then make specific policy proposals to address it.
The Surgeon General’s report is a typical artifact. The report first provides a comprehensive review of evidence for the negative health impacts of social isolation, citing a wide variety of research in medicine and social sciences. It also explores the relationship of connection to broader social themes such as community safety, local economic growth, and civic engagement:
Higher levels of social connection are associated with increased levels of civic engagement (defined as “actions to address issues of public concern”) and more representative government. Emerging evidence has shown that civic engagement helps to develop “empathy, problem solving, [and] cooperation” among community members. One study showed that higher levels of family and community connection during adolescence predicted civic engagement outcomes in young adulthood including a greater likelihood of voting and involvement in social action and conversation groups.
The report concludes with a national policy strategy, including a host of recommended programs. The programs include:
- Urban design policies to grow local interactions
- Mobilizing the health sector
- Strengthening local social infrastructure through volunteer programs and access to other social groups
- Linking lonely individuals to community-based organizations
- Reforming digital technology
- Coordinating a national research and advocacy agenda
- Developing stronger measurement instruments
These proposals track many of the recommendations made by Julianne Holt-Lunstad, the most cited researcher on this topic, in her 2017 article “Advancing social connection as a public health priority in the United States.”
Policy recommendations such as these generate budgets for grants and research agendas within government arms like the NIH. Resources flow through the government to universities and charities, as well as through NGOs like the World Health Organization and private foundations who take up the issue.
Two projects in Australia are typical examples of government-sponsored programs aiming to alleviate isolation among older people through social interventions. The G’day Line is a national support line where elderly people can have an anonymous conversation with a caring listener. Village Hubs are effectively a grant program for community-organized events and programming for the elderly in urban areas. These are not retirement homes; the Village Hub is just a layer of programming on top of an already existing community. Funding from these programs, from what I can tell, comes from the Australian Medicare budget.
Funding also comes from private foundations like the Robert Wood Johnson Foundation, which has allocated philanthropic dollars to researchers and to orgs conducting interventions like the Foundation for Social Connection. Ultimately these resources trickle down to specific people and organizations conducting local interventions, like Jared Siede and his Los Angeles-based organization Center for Council, which enacts local programs around building communication skills, mindful listening, and leadership.
3. Private Sector
The loneliness concept has also been picked up by entities in the private sector. The media has an important role to play here, turning policy statements into public discourse. The New York Times devoted 12 articles and opinion pieces to the “loneliness epidemic” in the last year alone. These articles frequently restate usual statistics and talking points like Holt-Lunstad’s “equivalent to 15 cigarettes,” and rehearse the interventions promoted by the public sector: limiting time spent online, being kind to one another, bolstering fraying community organizations, and so on.
Businesses are also reorienting themselves around the loneliness discourse. The notion of “the loneliness problem” is particularly appealing to startup founders. It can be used with investors to demonstrate a large addressable market in pitch meetings, yet also with the public and employees to foster a sense of social purpose. Othership, the Toronto-based bathhouse, cites the concept in its organizing values statements. The business Peoplehood, which runs empathic conversation and listening groups, lists a statistic about the number of people who identify as lonely on its website. The real estate development company Salt Lake Crossing makes use of the idea in their brand messaging and when speaking with journalists.

Some people view this trend with suspicion. But the elevation of loneliness to a public health problem clearly gives these organizations language for the social purposes they aim to address.
4. Individuals
Finally we turn to the lonely people who are the very reason for the loneliness apparatus.
It’s hard to say how the promotion of loneliness as a public health concern affects these individuals. But we have no choice but to offer a few speculations.
If you watch the NYT video linked above, you’ll get a sense of people who are truly lonely. Many of them cry in their calls with the reporters who documented their sadness. In gaining some public recognition that loneliness is real and affects many of them, perhaps some solace is reached, or more optimistically, they may be made aware of programs designed to alleviate isolation.
But not all people have this kind of self-awareness. The “loneliness epidemic” is sometimes also referred to as an “invisible crisis,” one that can’t be seen. I presume the reason for this is that most people are not entirely aware that they are lonely, or don’t even want to describe themselves that way. To be lonely is to be vulnerable. Some tentative evidence for this is the emphasis on destigmatizing loneliness and isolation found in the UK and USA government reports on the subject. In this matter “loneliness” is following the path set out out by “mental health” before it. The purpose of all this public messaging is to make people identify as “having it.”
If such campaigns are as effective as the mental health apparatus has been, the effects on individuals of destigmatizing and promoting loneliness will undoubtedly be loneliness salience: to make those who feel lonely more aware of their feelings and therefore more likely to take action. They may decide to join a social group in their city, participate in one of the many publicly-funded interventions, or visit a business with social wellness focus.
But here is exactly where we have to end our overview and speak in evaluative terms about the loneliness apparatus. The mental health apparatus created a nation of mental health-havers. If the loneliness apparatus is equally successful, could it create a society of the lonely?
The Convenience of Loneliness
Loneliness is an empirical fact, but the loneliness apparatus appears to be a solution to a problem—to many problems. Rising welfare costs, aging populations, urbanization, the disintermediation of local life by social media, and the continuing dilapidation of civic and social institutions are all real. With the exception of social media, none of these are new problems. What is new is how the concept of loneliness is being used to address all of them at once. This is why, I feel, there is something not-even-wrong about the entire concept. The policy proposals make nearly too much sense. As a friend said, they make your eyes glaze over when you read them.
These programs might have been found at any time in the last thirty years or more. Loneliness is not the cause of problems such as civic disengagement; obviously, the opposite is true. It is the fraying of social institutions and the rise of internet social media that have created mass social isolation. Yet locating the symptoms of these ills in the individual person, as this public health campaign rhetorically does, is bound to have an effect. It determines not only the type of intervention proposed, but also the attitudes of individuals who internalize a loneliness diagnosis. This may not only affect already lonely people, but also people with behavioral and emotional blockages who might otherwise conceive of themselves as “depressed” or “anxious.” The loneliness campaign implicitly endorses a self-diagnosis of “lonely” in addition to the mental health framing.
That individuals will internalize the diagnosis in this way, we have to assume, is the exact bet being made here. The mental health apparatus functions similarly. It insists on a dualist metaphysics and assigns causal power to the mind/brain of the individual. It then sees the mind/brain as the intervention pathway to restoration, whether through CBT, emotional work, or pharmacological treatment. By any standard this has been an enormously influential framing. The messaging has worked; “mental health” has become internalized as an unquestioned part of our culture. It seems normal to us to get a therapist or psychiatrist.
So it seems to me that a similar playbook is being run on “loneliness.” The bet is that individualizing these larger social problems as “loneliness,” and leveraging science’s authority to medicalize social connection, will indeed lead to behavior change on the part of individuals—more behavior change than similar policy programs would otherwise accomplish. By framing isolation as unhealthy as a pack of smokes, or comparing it to diet, individuals may take more responsibility for their social lives.
I don’t mean to assert some big conspiracy here. In all likelihood this “playbook” is being run because it’s the only one the public sector knows how to play. Everything about this rollout mimics the way “mental health” was brought to public attention, with few net new policy interventions. Yet there is a confluence of interests at play. Loneliness is a very convenient idea for addressing preexisting issues related to urban life, the elderly, poor populations, growing welfare costs, and mental health. It is really because loneliness is being inflated to touch all of these at once that I think it has been landed on, at least in the USA.
And this convenience gets at why the concept feels unfit for purpose. My friend Dan Taeyoung came up with a thought experiment to understand why “loneliness” feels so off. What if instead of the “loneliness epidemic,” the framing was the “being indoors epidemic” or the “conflict aversion epidemic?” These are two related issues. The first speaks to the excessive time spent inside and on screens rather than in social life outside. It even comes with similar Scientific™ studies about the health benefits of being in nature. The second is more radical, proposing that we have a culture of scared and invulnerable conflict avoiders who do not come into true contact with one another, bonding less while also being less tolerant and socially flexible. Both framings here are related to loneliness, yet have quite different affordances when it comes to designing solutions. Policies might include national hiking subsidies, the creation of a new class of social workers called Field Trip Workers, and the introduction of an Urban Green Space Indicator as a national quality of life metric. The second idea suggests nationally sponsored conflict mediation trainings, or the elevation of encounter groups to the status of evidence-based therapy.
These ideas are pretty harebrained. But here’s one more. If urban zoning is indeed one of the factors isolating both elderly and young people, why not frame the issue as a zoning crisis? Dan’s thought experiment points to the contradictions implicit in the loneliness apparatus. The framing of “loneliness” dismisses the truly challenging problems where traction is most important. Regulatory hurdles, entrenched actors, and powerful incentives dissuade from focusing on issues like zoning or social media regulation. But this is another way the loneliness apparatus follows mental health. The symptoms themselves are presented as the root cause, and given the label of diagnosis.
The thought experiment also shows how important it is for local organizers and businesses to find different idioms than “loneliness” for framing their social projects. “Solving loneliness” is like “solving mental health:” a fool’s errand. It’s counterproductive to think this way. In my experience, it is the positive content of a social group that motivates repeat participants and grows bonds. Ignoring the positive content leads to well-known but rather tired formats such as group dialogue and listening circles, which certainly have a role to play but which won’t resuscitate local life on their own. The most healing social spaces do not even make loneliness or “care” salient; they are intrinsically joyful to be part of, whether their context is religious, sporting, creative, or educational.
The social patterns of welcoming and enervating spaces need more creativity and attention. This is not something a national playbook is suited to address, but the best organizers and teachers know well. At the level of implementation, the negative term (“loneliness”) ought to be deemphasized in favor of the positive social content. I’ll end with a couple examples.
A few years ago, my colleagues and I co-authored an essay called Squad Wealth which extolled the benefits and creative potentials of friendships bonded through their group chats. Each section demonstrated a different characteristic of the squad: its shared lore and language, the camaraderie formed through taking on greater challenges together, and the potential to earn a living through squad activities. Importantly, the essay was written in a comical and youthful tone, a genuine expression of the joy we found in our own friendships. The essay went viral on publication, and we’ve since received countless messages from younger people who were inspired to start or strengthen their own squads after reading. This could only happen because we primarily spoke to the positive social force of friendship, rather than to its absence. It could certainly be argued that whatever energy we unleashed failed to address the loneliest individuals. But I think it’s more beneficial for those individuals who responded to us saying they realized they need a squad to have a clear notion of what to aim for, rather than simply having their loneliness highlighted.
A second example concerns spaces that do make healing and care central themes. While talk therapy nearly always addresses resistances and challenges in relationship to others, one-on-one therapy doesn’t address social isolation directly. Group talk therapy modalities have also fallen out of popularity. But the recent trend of “social wellness” gives me reason for optimism. I’ve only heard this term used by wellness entrepreneurs to describe the nascent category of health-forward social experiences. The recent surge of bathhouses and saunas is one example, as are social listening experiences like Floating. The growing popularity of different types of group yoga and wellness retreats could also be considered part of this trend. Interpersonal elements are considered a main ingredient for social wellness, but are not a hyperfixation.
To speak about cultural determinants of health is to speak about language. When the government chooses to devote resources to a concept like “loneliness,” not only does it endorse and subsidizes certain types of intervention, but it changes the meanings of health for our culture at large. It takes time for these meanings to settle into the soul of a nation. Luckily that gives ample time for reframing and retranslation. Therapists, social organizers, and businesses will no doubt come to understand the very real detriments of social isolation. But this is just the start of the conversation we must have on the terms of our culture of care.
Thanks to Dan Taeyoung, @qorprate, and Aaron Z Lewis for conversations that informed this piece.
Member discussion